>7 billion
clinical lab tests performed each year

The evolution of digital healthcare technologies continues to reshape care models, provider and consumer experiences, and healthcare operations. In recent years, we’ve seen an acceleration of technological advancements that has shifted the point-of-care from in-person office visits to virtual telehealth check-ins and remote monitoring via wearable devices. An analysis by Frost & Sullivan found that the telehealth market in the United States was predicted to display seven-fold growth by 2025.¹ The progression of new, innovative care models is just one of the reasons behind the ever-increasing amount of health-related data generated across the care continuum, including clinical data.
From diagnoses to lab results to vital signs, clinical data contains rich information about an individual’s health journey and includes timely, precise indicators that are not always present in other data sources, such as claims data. When leveraged strategically, high-quality clinical data can be a powerful tool. It has the potential to help payers reduce healthcare costs by closing critical gaps in care, increasing patient engagement, benefiting utilization, and ultimately improving long-term health outcomes and HEDIS® scores.
However, a majority of raw clinical data could potentially be unusable due to inconsistencies in formatting and completeness across electronic information systems. Achieving data interoperability and the ability to access and process data from multiple sources without losing meaning is top of mind for healthcare organizations. Health plans’ fervor to comply with the Centers for Medicare & Medicaid Services (CMS) Interoperability and Patient Access Final Rule, a requirement for certain payers to build standardized interfaces to exchange data with other payers, has spurred the adoption of Fast Healthcare Interoperability Resources (FHIR®) standards in the healthcare industry. While FHIR offers many benefits, it doesn’t solve the challenge of deriving value from legacy clinical data that is inconsistently collected and coded. For example, one clinician might document a flu shot in the procedures section of an electronic health record (EHR) while another might use a narrative note. This lack of standardization can lead to gaps in care and decision making based on fragmented information.
“Despite health plans having an endless amount of data seemingly at their fingertips, only a fraction of it can be leveraged to its full capacity due to the lack of consistency in data capture, format, and exchange capabilities.”
Standardizing data is just one step in the clinical data integration process. To effectively use clinical data as a strategic asset, the content that makes up the data and how it’s structured must be parsed, semantically normalized, enriched, and synthesized. Conquering this feat of interoperability that allows two or more systems to easily communicate and exchange data between one another requires a set of specialized skills and capabilities to deliver value at scale.
Proactive payers looking to gain a competitive edge while remaining compliant are turning to trusted vendors, like Availity. Availity has the experience and expertise to transform raw clinical data into a standard base like FHIR, and perhaps most importantly, can help solve quality issues and content challenges around complex coding variations.
“To effectively use clinical data as a strategic asset, the content that makes up the data and how it’s structured must be parsed, semantically normalized, enriched, and synthesized.”
Government regulations are advancing the urgency surrounding interoperability and FHIR. Organizations are realizing two critical challenges:
Healthcare data volumes are increasing exponentially year-over-year, generating massive amounts of data points from EHRs, government registry results, and lab values.
Today, clinical data from siloed sources across the industry exist in various formats, both standard and non-standard, and FHIR is only just gaining mainstream acceptance. While many new emerging datasets are being generated in the FHIR standard, a significant amount of historical data exists in Health Level Seven® International Version 2 (HL7® V2), Consolidated Clinical Document Architecture (C-CDA), and custom formats. To think about it holistically, every lab result is an HL7 V2 message.
There are more than seven billion clinical lab tests performed in the U.S. each year.² As for C-CDA, every patient encounter with the healthcare system generates hundreds of documents in the C-CDA format, resulting in over 500 million C-CDA documents being exchanged annually in the U.S.³ With the summation of all this data, experts predict that the global datasphere will grow from 33 zettabytes in 2018, to 175 zettabytes by 2025.⁴ To successfully leverage FHIR to its full potential, organizations must first convert legacy data sources. This conversion process is incredibly complex because of the evolving FHIR specifications and lack of a one-to-one crosswalk from other standard formats.
clinical lab tests performed each year
C-CDA documents exchanged annually
global datasphere by 2025
Having specific expertise in the HL7 and continuously maintaining, testing, and applying mappings for C-CDA to and from FHIR R4 US Core are vital components of a successful conversion process. That’s why health plans, government agencies, and other stakeholders are turning to innovative companies like Availity to help accelerate their FHIR strategy by combining conversion complexities with the need to scale and automate such a process.
HL7 V3 Act Status (from C-CDA) map to FHIR statuses. Even for a small and relatively well-defined value set, there can be significant complexities. First, the mappings are different for different FHIR resources that have unique value set requirements. Second, the same C-CDA status can map to none, one, or multiple FHIR status
For organizations with the ability to convert and produce data in FHIR, the challenge is then with semantic interoperability, as the FHIR standard alone will not correct inaccurate, incomplete, or inconsistent source data. Varying documentation from provider to provider and practice to practice as well as inconsistent use of standard terminologies leads to incredible content variation within clinical sources. A single lab test, associated with one standard Logical Observation Identifier Names and Codes (LOINC), may have more than 100 different local codes and descriptions, based on how the test is documented. Without addressing these inconsistencies, organizations risk perpetuating the use of poor-quality clinical data in FHIR. As one Continuity of Care Document (CCD) may generate over 450 FHIR resources, the number of poor-quality data being exchanged between care teams, delivered directly to patients, and used to inform care, increases significantly.
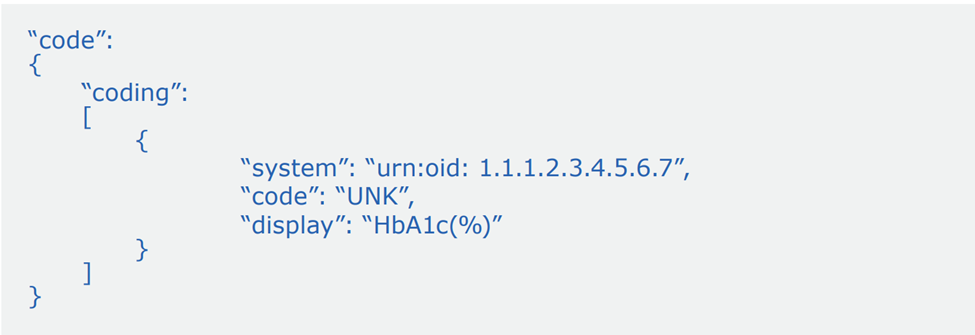
The example below represents a single lab test documented within a CCD without a standard code and the perpetuated gap in the converted FHIR resource
Incomplete and inaccurate data in CCD format…

…will be incomplete and inaccurate data in FHIR format.
In fact, a majority of raw clinical data sources may contain incomplete and inaccurate data due to missing, conflicting, or invalid elements. Thus, to effectively leverage FHIR to meet government mandates, improve care quality, increase analytics accuracy, or differentiate, organizations must address semantic normalization and quality improvement
As health plans prioritize compliance with CMS mandates and organizations across the industry advance respective interoperability and FHIR initiatives, best of breed technology partners are emerging to solve challenges pertaining to clinical data usability with clinical informatics expertise. Availity Fusion generates “Upcycled Data”, a term we use to describe clinical data that’s ready to use to uncover solutions, elevate efficiency, and deliver smarter care.
Availity’s fast and scalable API technology transforms high volumes of multi-source, multi-format clinical data into an interoperable and flexible data asset. Achieved using our Upcycling Data™ technology to improve data quality, Availity Fusion offers real-time and scalable FHIR conversion to produce high-quality FHIR resources on demand. The HL7 community recognizes the importance and challenge of this work and has launched a working group project initiative focusing on mapping C-CDA to FHIR and back. Availity is co-leading this initiative. Our dedicated team members engage with standards experts and industry leaders to share and discuss mapping approaches and examples. Availity hosts weekly sessions, as well participates in FHIR Connectathons, to drive the alignment efforts on the best practices. The mappings and aligned sample artifacts will serve as basis for a future ballot, which is the HL7 process for the public to express their comments and opinions on the proposed specification.
“Availity’s fast and scalable API technology transforms high volumes of multi-source, multi-format clinical data into an interoperable and flexible data asset.”
To empower customers and partners with enhanced FHIR data for better data exchange and decision-making, Availity’s FHIR portfolio consists of the following:
Leveraging a deep bench of clinical informaticists, with extensive involvement in the FHIR community and leadership in HL7’s initiative surrounding C-CDA to FHIR mapping, Availity converts legacy data sources, including C-CDA, HL7 V2 messages, and flat files, to FHIR resources in near real-time.
Information may be presented in different formats or use different terminologies. For example, systems using Systematized Nomenclature of Medicine Clinical Terms (SNOMED CT) codes, Current Procedural Terminology (CPT) codes, local codes, or free text to refer to one procedure. Our API-based Upcycling Data technology, supports data upcycling by aggregating data from EHRs, health information exchanges, labs, and other sources and then normalizing and enhancing it to deliver a consistent, standards-based data asset that’s ready for use.
To support increasing customer volumes, Availity’s FHIR conversion is scalable up to millions of CCDs per day. Availity loads CCDs at a rate of ~2M CCD/day and 10 million HL7 V2 messages per day, with consistent processing speeds of 0.66 seconds/CCD. For a single production customer, 900,000 CCDs and 10-15 million HL7 V2 messages are processed per day, producing more than seven billion FHIR resources to date to enable downstream use cases.
Post-implementation, Availity Fusion’s data quality improvement and FHIR conversion capabilities are entirely automated and do not require human intervention.
To flexibly integrate into a variety of data architectures, Availity offers APIs or real-time FHIR eventing capabilities, streaming updated patient data as it is available
Availity goes beyond FHIR conversion and even simple terminology mapping to ensure that multi-format clinical data is semantically normalized and ready for use. Today, health plans, government agencies, health information exchanges, and other organizations across the industry leverage these capabilities to help achieve FHIR compliance and interoperability. Implementing a real-time, scalable FHIR solution can help position these organizations for growth and agility in the future world of FHIR.